GENERAL
GENERAL
Sphenopalatine ganglion is a parasympathetic ganglion, no more than 5mm in width, located in the pterygopalatine fossa of the skull. The sphenopalatine ganglion sends nerve fibres to the lacrimal glands, glands of the nasal cavity, paranasal sinuses, palate and upper pharynx. Postganglionic sympathetic fibres and afferent somatosensory branches of the maxillary nerve pass through the sphenopalatine ganglion without terminating there. All postganglionic parasympathetic and sympathetic branches, as well as all afferent somatosensory branches, can be blocked with the application of sphenopalatine ganglion block.
INDICATIONS
• Cluster headache
• Atypical prosopalgia
• Trigeminal neuralgia
 TECHNIQUE
TECHNIQUE
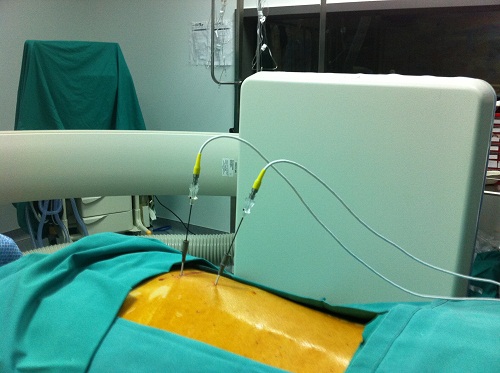
The patient is placed in the supine position, with head stabilized on a doughnut-cushion. The pterygopalatine fissure (that looks like a vase turned upside down) is localized under fluoroscopic guidance. Above the fissure lies the sphenoid sinus and below is the maxillary sinus. The needle entry site is targeted with a metallic indicator and is identified right below the zygomatic arch. After applying local anaesthesia, a blind needle, 10cm long, is slowly advanced frontwards and upwards through an inserter. The fluoroscopic view is directed posterolaterally and the needle is advanced until it meets the nasal wall.At this exact point the drug solution is injected.
The same technique is followed when radiofrequency is applied to the ganglion. The only difference is that a special needle and electrode are used, with the electrode being inserted through the needle. The ganglion is stimulated with a sensory testing by using a radiofrequency generator and -once the ganglion identified- either conventional or pulsed radiofrequency is applied. During the sensory testing, the patient experiences paraesthesia that should be localized at the sides and the posterior nasal wall, with low voltage electric current. There should not be paraesthesia induced in the soft palate or maxilla because this would indicate that the tip of the needle is near the maxillary nerve or near a branch of this nerve. If conventional radiofrequency is applied in such a case, it is the maxillary nerve that will be ablated instead of the sphenopalatine ganglion. Should pulsed radiofrequency be applied, even if the tip of the needle is wrongly placed, no harm will be done. (1-21)
LITERATURE
1. Ferrante FM, Kaufman AG, Dunbar SA, Cain CF, Cherukuri S. Sphenopalatine ganglion block for the treatment of myofascial pain of the head, neck, and shoulders. Reg Anesth Pain Med. 1998 Jan-Feb;23(1):30-6.
2. Janzen VD, Scudds R. Sphenopalatine blocks in the treatment of pain in fibromyalgia and myofascial pain syndrome. Laryngoscope. 1997 Oct;107(10):1420-2.
3. Manahan AP, Malesker MA, Malone PM. Sphenopalatine ganglion block relieves symptoms of trigeminal neuralgia: a case report. Nebr Med J. 1996 Sep;81(9):306-9.
4. Morelli N, Mancuso M, Felisati G, Lozza P, Maccari A, Cafforio G, Gori S, Murri L, Guidetti D. Does sphenopalatine endoscopic ganglion block have an effect in paroxysmal hemicrania? A case report. Cephalalgia. 2009 May 5.
5. Narouze S, Kapural L, Casanova J, Mekhail N. Sphenopalatine ganglion radiofrequency ablation for the management of chronic cluster headache. Headache. 2009 Apr;49(4):571-7. Epub 2008 Sep 9.
6. Olszewska-Ziaber A, Ziaber J, Rysz J. [Atypical facial pains–sluder’s neuralgia–local treatment of the sphenopalatine ganglion with phenol–case report] Otolaryngol Pol. 2007;61(3):319-21. [Article in Polish]
7. Peterson JN, Schames J, Schames M, King E. Sphenopalatine ganglion block: a safe and easy method for the management of orofacial pain. Cranio. 1995 Jul;13(3):177-81.
8. Prasanna A, Murthy PS. Vasomotor rhinitis and sphenopalatine ganglion block. J Pain Symptom Manage. 1997 Jun;13(6):332-8.
9. Quevedo JP, Purgavie K, Platt H, Strax TE. Complex regional pain syndrome involving the lower extremity: a report of 2 cases of sphenopalatine block as a treatment option. Arch Phys Med Rehabil. 2005 Feb;86(2):335-7.
10. Raj P, Lou L, Erdine S et al. Radiographic imaging for regional anesthesia and pain management. New York, Churchill Living-stone, 2003, pp 66-71.
11. Robiony M, Demitri V, Costa F, Politi M. [Percutaneous maxillary nerve block anesthesia in maxillofacial surgery] Minerva Stomatol. 1999 Jan-Feb;48(1-2):9-14. Italian.
12. Saberski L, Ahmad M, Wiske P. Sphenopalatine ganglion block for treatment of sinus arrest in postherpetic neuralgia. Headache. 1999 Jan;39(1):42-4.
13. Sanders M, Zuurmond WW. Efficacy of sphenopalatine ganglion blockade in 66 patients suffering from cluster headache: a 12- to 70-month follow-up evaluation. J Neurosurg. 1997 Dec;87(6):876-80.
14. Stechison MT, Brogan M. Transfacial transpterygomaxillary access to foramen rotundum, sphenopalatine ganglion, and the maxillary nerve in the management of atypical facial pain. Skull Base Surg. 1994;4(1):15-20.
15. Varghese BT, Koshy RC. Endoscopic transnasal neurolytic sphenopalatine ganglion block for head and neck cancer pain. J Laryngol Otol. 2001 May;115(5):385-7.
16. Waldman S. Atlas of Interventional Pain Management. Philadelphia, WB Sanders, 1998, pp 10-12.
17. Waldman, S. Sphenopalatine ganglion block- 80 years later. Reg Anesth 1993; 18:274-276.
18. Waxman, S. Correlative Neuroanatomy, 23rd ed. Stamford, Appleton & Lange, 1996. Pp 265-266.
19. Windsor RE, Jahnke S. Sphenopalatine ganglion blockade: a review and proposed modification of the transnasal technique. Pain Physician. 2004 Apr;7(2):283-6.
20. Windsor R, Gore H, Merson M: Interventional sympathetic blockade. In Lennard T (ed.) Pain Procedures in Clinical Practice, 2nd ed. Philadelphia, Hanley & Belfus, 2000, pp 321-324.
21. Yang Y, Oraee S. A novel approach to transnasal sphenopalatine ganglion injection. Pain Physician. 2006 Apr;9(2):131-4.